Introduction
You have probably seen movies or TV shows that portray dissociative identity disorder as something scary or dramatic. A character switches between personalities in an instant, often with a Hollywood twist. The truth is far less sensational and much more human.
Dissociative identity disorder, or DID, is a real mental health condition where a person experiences two or more distinct identity states. It is one of the most misunderstood conditions in the field of mental health. Many people confuse it with antisocial personality disorder or assume it is the same as borderline personality disorder symptoms. These mix-ups add to the stigma and make it harder for people to get the right help.
The numbers might surprise you. Research shows DID is not as rare as experts once thought. For example, studies have found that dissociative identity disorder appears in 4 percent to 7.5 percent of patients in psychiatric hospital settings, according to facts and statistics on DID. In outpatient clinics, the rate ranges from 2 to 6 percent. And in the general population, about 1.5 percent of adults may have the condition, though many remain undiagnosed or misdiagnosed for years.
Why does this matter? Because accurate, research-backed information is essential. It reduces shame, helps people recognize symptoms in themselves or loved ones, and guides them toward proper care.

Whether you are learning for yourself or to support someone else, understanding the dissociative spectrum is a powerful first step.
This article provides a clear, evidence-based overview of dissociative identity disorder, how it connects to related personality disorders, and what real recovery looks like. No Hollywood drama just useful facts that can change how you see this condition.
If you want to stay connected with more mental health news and supportive resources, you can Join The Newsletter for ongoing wellness updates and community insights.
What Is Dissociative Identity Disorder? Core Symptoms and DSM-5-TR Criteria
So what does dissociative identity disorder actually look like in real life? The official answer lives in the DSM-5-TR, the manual mental health professionals use to diagnose conditions. And the criteria might surprise you.
The two main features
The DSM-5-TR outlines two core symptoms that must be present for a DID diagnosis.
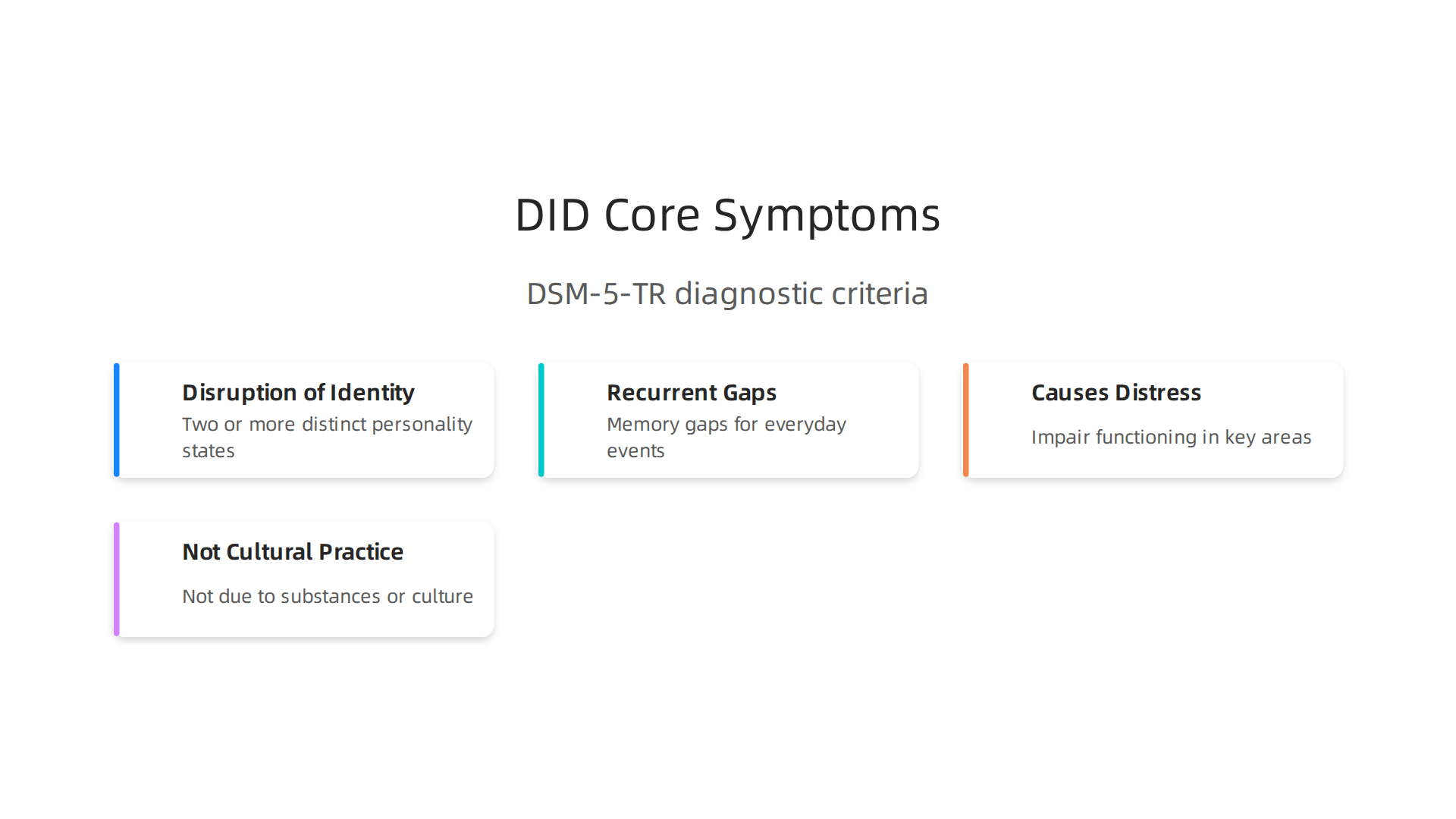
First, there is a disruption of identity. This means a person experiences two or more distinct personality states. Each one has its own way of perceiving, relating to, and thinking about the world and the self. Some cultures describe this as a possession experience, but the key is a marked discontinuity in the sense of self and sense of agency. These shifts can be observed by others or reported by the person themselves, according to the official DID in the DSM-5 criteria.
Second, there are recurrent gaps in memory. This is not ordinary forgetfulness like misplacing your keys. It involves gaps in recall of everyday events, important personal information, or traumatic experiences that do not fit normal forgetting patterns. Someone might not remember a conversation they had an hour ago or a significant life event from years back.
For the diagnosis to apply, these symptoms must cause real distress or problems in social, work, or other important areas of life. And the symptoms cannot be part of accepted cultural or religious practices or caused by substances or medical conditions, as outlined in the symptom description from the American Psychiatric Association.
Where DID comes from
Here is one of the most important things to understand about this condition. DID does not appear out of nowhere. Research consistently links it to severe, chronic childhood trauma, often abuse that begins before age six. The mind copes with overwhelming experiences it cannot escape by separating them from the main sense of self. This is not weakness. It is a survival strategy that helped a child get through unbearable situations.
The National Institutes of Health explains that dissociative identity disorder is associated with severe behavioral health symptoms and is firmly rooted in early trauma history.
The identities or alters are not new people; they are fragmented parts of one person that were never able to integrate during childhood.
Clearing up the biggest myth
People often confuse DID with schizophrenia. This is one of the most stubborn misconceptions in mental health. Schizophrenia involves psychosis, meaning a person may lose touch with reality through hallucinations or delusions. DID does not involve psychosis. It involves fragmentation of identity. A person with DID knows that their memory gaps and identity shifts are happening, which is different from someone experiencing a break from reality.
This confusion causes real harm. It delays proper diagnosis and treatment. Many people spend years being treated for other conditions before someone recognizes the dissociative identity disorder.

In fact, the International Society for the Study of Trauma and Dissociation reports that people may spend 5 to 12 years in treatment before receiving an accurate DID diagnosis.
Why the DSM-5-TR update matters
The latest version of the diagnostic manual made some helpful updates. It expanded Criterion A to include possession-form phenomena, which makes the criteria more culturally inclusive. It also clarified that memory gaps can occur for everyday events, not just traumatic ones. These changes help clinicians identify DID in a wider range of people and reduce the risk of misdiagnosis.
Understanding these core symptoms and criteria is the foundation. Once you know what DID actually is, the next step is recognizing how it shows up day to day and what real support looks like.
The Spectrum of Dissociative Disorders: Beyond DID
DID gets most of the attention, but it is not the only condition where the mind disconnects from itself. Dissociative disorders come in several forms, and they share a common thread: a breakdown in how a person experiences consciousness, memory, identity, or perception.
Understanding the full spectrum helps you see that dissociative identity disorder is one part of a bigger picture.
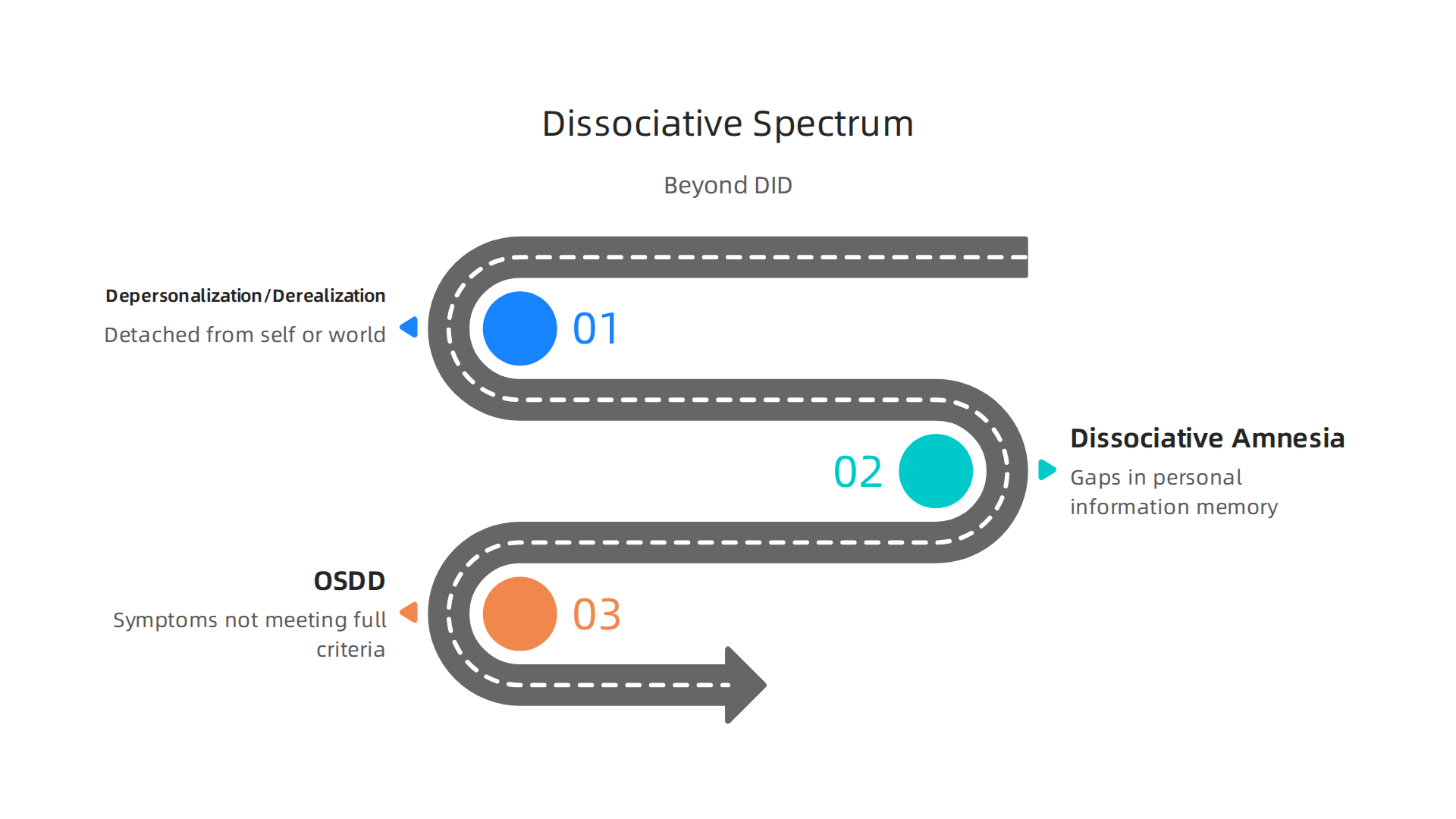
Depersonalization / Derealization Disorder
This condition is all about feeling detached from yourself or the world around you. With depersonalization, you might feel like you are watching your own life from outside your body. With derealization, the world feels dreamlike, foggy, or unreal. The key difference from DID is that your sense of identity stays intact. You know who you are, but something feels off. These experiences can be terrifying, especially when they happen out of nowhere. The DSM-5-TR recognizes this as a separate diagnosis that does not involve distinct personality states.
Dissociative Amnesia
Dissociative amnesia is more than normal forgetfulness. It involves gaps in memory for personal information, often linked to trauma. A person might block out entire periods of childhood or forget a specific event. Unlike the amnesia in DID, here there are no alternate identities. The memory loss itself is the main problem. In some cases, people with dissociative amnesia may also experience dissociative fugue, where they wander away from home and have no memory of how they got there. Research from the National Institutes of Health shows that dissociative amnesia is often missed because it can look like other conditions.
Other Specified Dissociative Disorder (OSDD)
This category catches people who have dissociative symptoms but do not fully meet the criteria for DID or other specific disorders. For example, someone might have identity disruption without amnesia, or have chronic depersonalization that does not meet the full criteria for depersonalization disorder. OSDD is actually more common than many realize. Studies suggest that rates for OSDD range from 0.2% to over 8% depending on the population, which means it affects a significant number of people.
The bigger picture
Dissociative disorders as a whole are underdiagnosed. Many people spend years cycling through treatments for anxiety, depression, or borderline personality disorder symptoms before someone recognizes the dissociation underneath. The more you understand about these conditions, the easier it is to spot them and seek the right kind of help.
If this topic resonates with you, you are not alone. Many people find that learning about dissociation opens a door to understanding themselves better. A great next step is to connect with a community that gets it. You can join the newsletter for ongoing insights and support as you explore your mental health journey.
Personality Disorders: An Overview of Clusters and Key Features
Now that you understand the dissociative disorders, let us look at another group that often gets mixed up with them. Personality disorders are lasting patterns of thinking, feeling, and behaving that differ from what your culture expects. The DSM-5-TR groups them into three clusters based on shared features.
Cluster A covers odd or eccentric disorders. This includes paranoid personality disorder, schizoid personality disorder, and schizotypal personality disorder. People with these conditions often seem detached or suspicious. They may struggle with trust and social connection. These disorders share some surface features with dissociative identity disorder but do not involve distinct identity states or amnesia.
Cluster B includes dramatic, emotional, or erratic disorders. This is the group most likely to be confused with dissociative identity disorder. Antisocial personality disorder, borderline personality disorder, histrionic personality disorder, and narcissistic personality disorder all live here. They involve unstable emotions, impulsive behavior, and trouble with relationships. The confusion with DID happens most often with borderline personality disorder.
Cluster C covers anxious or fearful disorders. Avoidant personality disorder, dependent personality disorder, and obsessive-compulsive personality disorder are part of this cluster. People with these conditions tend to feel tense, insecure, or overly controlled.
Why Borderline Personality Disorder Gets Confused with DID
Borderline personality disorder symptoms include identity disturbance, emotional swings, and fear of abandonment. These can look a lot like the identity shifts in dissociative identity disorder. But there is a key difference. In BPD, the identity disturbance is a constant feeling of not knowing who you are. In DID, the identity disruption involves distinct personality states with their own sense of self and agency. The Borderline personality disorder: a comprehensive review explains that BPD involves problems with self image that are stable and ego syntonic, while DID involves actual dissociation between identities.
Why Accurate Diagnosis Matters
Getting the right label is not just about paperwork. It changes treatment. BPD responds well to therapies like dialectical behavior therapy (DBT). DID requires trauma focused therapy that addresses the dissociative structure. Mistaking one for the other can lead to years of the wrong treatment. If you suspect either condition, a thorough evaluation by a professional who understands both is essential. Accurate classification leads to better outcomes and less wasted time.
DID vs. Borderline Personality Disorder: Key Differences and Diagnostic Challenges
You might hear someone describe feeling like they have different sides to themselves. That could point to dissociative identity disorder (DID) or borderline personality disorder (BPD). Both involve identity struggles and emotional ups and downs. But they are not the same condition.
Here is the core difference. In dissociative identity disorder, a person experiences distinct personality states. Each state has its own memories, behaviors, and sense of self. These states often come with gaps in memory, called amnesia. One part might not know what another part did. That is not what happens in BPD.
How BPD Shows Up
People with borderline personality disorder symptoms have an unstable sense of self. They may feel empty or confused about who they are. But that feeling is constant, not split into separate identities. The Borderline personality disorder: a comprehensive review points out that BPD identity disturbance is stable and ego syntonic. That means the person feels the confusion is part of them. In DID, the identity states are distinct and separate from each other.
BPD also brings intense fear of abandonment, stormy relationships, and rapid mood shifts. These can look like the switches between identities in DID. But in BPD there are no amnesia gaps and no fully separate personalities. The emotional swings happen within one continuous sense of self.
Why Misdiagnosis Happens
Both conditions can stem from childhood trauma. Both involve emotional dysregulation. So a clinician might mistake one for the other, especially during a short visit. A careful long term assessment is needed to tell them apart. Experts recommend watching how identity shifts happen over time. Does the person have clear memory gaps? Do they report feeling like different people with different names or ages? If yes, DID is more likely. If the identity confusion is more about feeling empty or not knowing yourself, BPD is the better fit.
Getting the Right Diagnosis Matters
Treatment paths differ a lot. DID responds best to trauma focused therapy that works with the dissociative structure. BPD often improves with dialectical behavior therapy. Mixing them up can waste years. If you or someone you know is struggling with identity symptoms, seek a professional who understands both conditions.

Staying informed about mental health news can also help you spot the signs early. If you want to keep learning and connect with others on this journey, you might find value in Joining The Newsletter for ongoing wellness insights and community support.
Treatment Approaches for Dissociative and Personality Disorders
Getting the correct diagnosis is a relief. But it is only the first win. The real work starts with finding a treatment plan that actually fits your specific condition. The paths for dissociative identity disorder and BPD look very different. Knowing which road to take makes all the difference in your recovery.
How Dissociative Identity Disorder Is Treated
The evidence based standard for DID is phase-oriented therapy. This approach breaks the long healing journey into three clear stages.
Phase one is all about safety and stability. You learn grounding techniques to stay present in the moment. You build coping skills to handle daily stress and strong emotions. You also work on building trust with your therapist and the different parts of yourself. Phase two focuses on processing the traumatic memories that led to the dissociation. This is done slowly and carefully to avoid overwhelming you. Phase three works on integration. The goal is to help the different parts of yourself work together as a team. This phase-oriented treatment for DID has strong research support showing real improvement over time.
Some people aim for final fusion, where all parts fully combine into one identity. Others find peace in functional multiplicity, where the parts remain but cooperate and share memories. Both paths are valid.
How Borderline Personality Disorder Is Treated
BPD has a different gold standard therapy. Dialectical behavior therapy, or DBT, is the approach with the most research backing it. DBT teaches four main skill sets: mindfulness, distress tolerance, emotion regulation, and interpersonal effectiveness. It helps people manage intense emotions without acting on impulse. Research confirms that DBT for borderline personality disorder reduces self-harm and improves daily functioning. Other therapies like mentalization based therapy and schema therapy also help. The key is finding a structured approach that fits your needs.
What About Medication?
No pill can directly fix dissociation or a personality disorder. But medication can help with the symptoms that come alongside these conditions. Things like depression, anxiety, or trouble sleeping can be managed with medication. As noted in the NHS treatment for dissociation, there is no specific drug for dissociation, but antidepressants can help with related conditions. Medication works best when paired with regular therapy.
Starting Your Healing Journey
Healing from DID or BPD takes time. It requires a therapist who truly understands your specific condition. And it requires support from people who get it. If you are ready to move from passive scrolling into real action, consider taking a brave first step. You could Join An Experiment that turns curiosity and courage into shared progress and connection.
Living with Dissociative Identity Disorder: Recovery, Hope, and Reality
If you have dissociative identity disorder or love someone who does, you have probably heard mixed messages about what life can look like. Some sources make it sound hopeless. Others promise quick fixes that do not hold up. The truth is more balanced and far more encouraging.
Recovery from dissociative identity disorder is not a myth. It takes time, the right support, and consistent effort. But many people get there. According to a guide on Living With Dissociative Identity Disorder: Before and After Treatment, people with DID can absolutely spend time with loved ones, keep working, and lead fulfilling lives. The key is finding the right treatment and sticking with it.
What does recovery actually look like? For some people, it means reaching a point where the different parts of themselves cooperate and share memories. This is often called functional multiplicity. Life becomes more stable. Emotions stay calmer. Relationships improve. For others, recovery means full integration, where all parts come together into one identity. Both paths are real. Both take work. And both are worth pursuing.
Community support makes a big difference. Feeling alone with DID can make everything harder. That is why psychoeducation and peer support matter so much. When you learn how DID works, the strange symptoms start to make sense. You stop feeling broken. You realize your mind was doing its best to protect you. Support groups, both online and in person, let you connect with others who get it. As explained in a Guide to Dissociative Identity Disorder, building a strong support network and educating yourself and others can reduce stigma and improve your day-to-day life.
Stigma is a real barrier. Sadly, many people never seek help because of how DID is portrayed in movies and on social media. A study on the perceived impact of misportrayals of dissociative identity disorder found that inaccurate media depictions lead to profound shame, delays in getting treatment, and even mistreatment by healthcare providers. When you grow up seeing your own condition shown as scary or fake, it is hard to reach out. But that stigma does not have to win. Accurate information and compassionate support can break through the fear.
Here is the honest truth: living with DID is not easy, but it is not a life sentence. Many people learn healthy coping skills, build strong relationships, and find joy.

You deserve that same chance.
If you are ready to stop scrolling and start connecting with a community that gets it, consider taking a small step. You could Join The Newsletter to receive ongoing updates, encouragement, and opportunities to participate in something bigger. You are not alone in this journey.
Summary
This article offers a clear, research-based guide to dissociative identity disorder (DID), explaining what it looks like, where it comes from, and how it fits within the broader dissociative spectrum and personality disorders. It summarizes the DSM-5-TR diagnostic criteria—identity disruption and recurrent memory gaps—notes the strong links to early, severe childhood trauma, and clears up frequent confusions with schizophrenia and borderline personality disorder. The piece outlines related conditions (depersonalization, dissociative amnesia, OSDD), highlights DSM updates that improve cultural sensitivity, and describes how diagnosis affects treatment choices. It then contrasts phase-oriented therapy for DID with DBT for BPD, reviews the role of medication, and offers a realistic view of recovery including functional multiplicity and integration. Readers will finish able to recognize key symptoms, understand why accurate diagnosis matters, and know which treatment approaches to seek or discuss with a clinician.