Introduction
You have probably heard the term "multiple personality disorder" before. Maybe you saw it in a movie or read it in a news article. The truth is, most of what we think we know about this condition is wrong.
Multiple personality disorder (MPD) is not what Hollywood shows you. Clinically, it is now called dissociative identity disorder (DID). It belongs to a group that includes cluster B personality disorders, but it works very differently. The name change is not just a simple synonym swap. It reflects a deeper medical understanding of what is really happening inside the mind.
Here is what this article will do for you. First, it will clear up what MPD actually is and what it is not. Second, it will separate real symptoms from fiction. And third, it will explain how the mental health act and other laws shape the way people with this condition get care.
By the end, you will have a much clearer picture of multiple personality disorder and the legal protections that exist for those who live with it every day.

If topics like this matter to you, Join The Newsletter to stay connected and keep learning.
Let us start by looking at how we got from MPD to the name doctors use today.
What Is Multiple Personality Disorder? (Clinical Understanding in 2026)
In 2026, doctors almost never say "multiple personality disorder." That name belonged to an older idea of separate people living in one body. The real condition is called dissociative identity disorder (DID), and it works very differently.
First, let’s clear up a big mix-up. DID is not a personality disorder. It belongs to the dissociative disorders family, not the cluster B personality disorders group. In fact, a medical overview of the condition confirms that DID is not one of the ten personality disorders listed in the DSM-5-TR. This matters because personality disorders involve long-term patterns of behavior, while DID involves a split in a person’s sense of self.
So what does DID actually look like? According to the official DSM-5 criteria for dissociative identity disorder, a person must show three main signs.
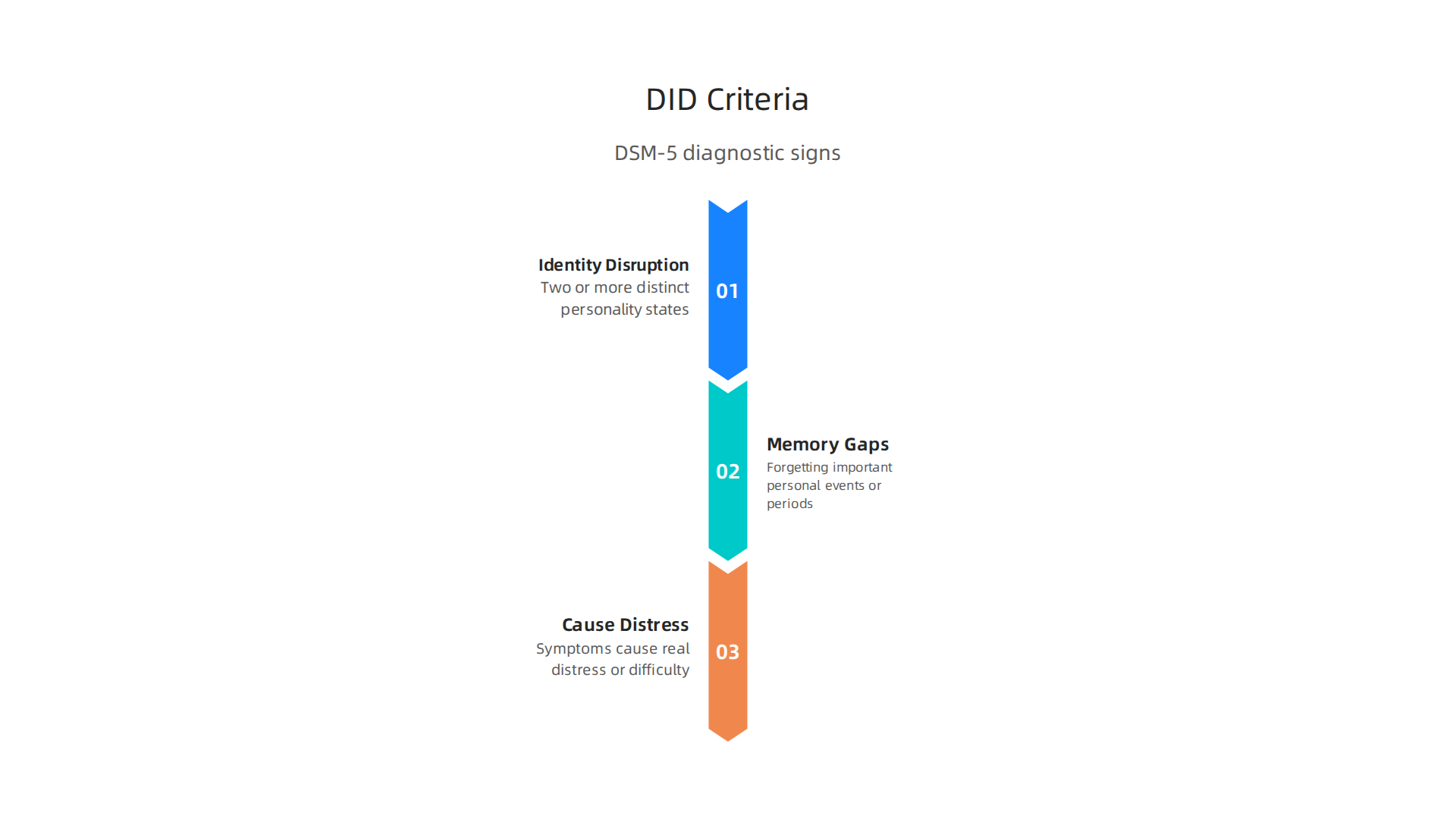
The first is identity disruption. This means having two or more distinct personality states. Each state can have its own way of thinking, feeling, and acting. The person may feel like a different version of themselves at different times. The second sign is memory gaps. These are not just forgetting where you put your keys. We are talking about forgetting important personal events or even entire periods of time. The third sign is that these symptoms cause real distress or make it hard to work, maintain relationships, or handle daily life.
How common is this? Research suggests that about 1 to 3 percent of people may meet the criteria for DID. That is roughly the same rate as schizophrenia. But many cases never get diagnosed. People often go years without understanding what is happening to them. They might think they just have a bad memory or mood swings.
This is why raising awareness matters. For anyone who wants a deeper walk through the symptoms and how they differ from other conditions, this detailed guide to DID symptoms and causes breaks it all down in plain language.

The key takeaway? Multiple personality disorder is not what TV shows make it out to be. It is a real, often misunderstood condition rooted in trauma. And thanks to updated diagnostic tools, more people can finally get the right help.
Dissociative Identity Disorder vs. Historical MPD – Key Differences
Here is a fact that surprises most people: the name "multiple personality disorder" stopped being the official diagnosis in 1994.
That was over 30 years ago. The American Psychiatric Association swapped it for dissociative identity disorder when they published the DSM-IV, and the change was not just about sounding more modern.
The old name gave people the wrong picture. It made the condition sound like someone had several complete personalities living inside them, each running the body like a shift worker. But that is not what the evidence shows. Modern research explains that DID is actually a trauma response, not a personality problem. A detailed review of multiple personality disorder and dissociative identity disorder confirms that the condition is tied to severe childhood trauma and involves a fractured sense of self, not separate people.
This is a huge difference. Cluster B personality disorders like borderline or narcissistic personality disorder develop from long-term patterns of behavior and thinking. DID comes from dissociation, which is the mind’s way of surviving unbearable experiences by splitting awareness. The two families of disorders are not the same, and mixing them up leads to bad treatment and more shame.
Why does this name change matter in 2026? Because words shape how we see ourselves and others. When someone hears "multiple personality disorder," they might picture something dramatic or scary. When they hear "dissociative identity disorder," they learn about a real condition rooted in real pain. This shift in language makes it easier for people to seek help without fear of being judged.
If you want to understand more about how the words we use affect mental health conversations, you can explore these mental health synonyms that reduce stigma. And if this topic matters to you and you want to keep learning about wellness and staying connected, Join The Newsletter for ongoing updates.
The History and Controversy of Multiple Personality Disorder
To understand why multiple personality disorder is still a loaded term in 2026, you have to go back to the 1970s. That is when the story of "Sybil" exploded into American culture and permanently shaped how the public sees this condition.
Sybil was actually Shirley Ardell Mason, an art teacher from Kentucky. Her life story became the 1973 book Sybil, which claimed she had 16 separate personalities living inside her. The book sold millions of copies. The 1976 TV movie starring Sally Field turned the story into a national conversation. Before Sybil, multiple personality disorder was almost never diagnosed. After Sybil, everyone thought they knew what it looked like.
According to the Wikipedia article on Shirley Ardell Mason, her therapist Dr. Cornelia Wilbur believed Mason developed multiple personalities to cope with severe childhood abuse at the hands of her mother. But from the start, questions surrounded the case.
The numbers tell a shocking story. A Retro Report video on the Sybil case explains that before this book and film, fewer than 200 cases of MPD had ever been reported in all of Western medical history. But after Sybil, diagnoses exploded. By the late 1980s, around 40,000 people in the United States alone had been diagnosed. That kind of jump does not happen naturally.
Critics raised serious concerns about what really happened in Wilbur’s therapy room. Psychiatrist Herbert Spiegel, who treated Mason while Wilbur was on vacation, believed that Wilbur was subtly guiding Mason to produce the symptoms. Journalist Debbie Nathan later published Sybil Exposed, arguing that the case was a deliberate fraud involving the patient, the therapist, and the writer. The CBC report on Sybil’s true family history explains how this controversy created a ripple effect that damaged trust in the entire diagnosis.
The controversy goes deeper than just one case. Questions about iatrogenesis, or therapists accidentally creating symptoms in their patients, became a major concern. The recovered memory debate of the 1980s and 1990s was fueled by cases like Sybil. Therapists faced lawsuits. The entire field of trauma therapy came under attack.
This history still matters for legal and clinical reasons today. Under the Mental Health Act, accurate diagnosis is critical for proper treatment and patient rights. When a diagnosis carries this much baggage, it affects how courts, doctors, and families respond to people who need help.
For anyone trying to make sense of these issues, understanding the full history helps separate real science from sensationalism. If you want a modern perspective on how this condition is understood today, the article on dissociative identity disorder symptoms and borderline personality disorder differences provides a clearer framework.
The Sybil story is not just a historical footnote. It is a warning about how media hype, professional bias, and a single dramatic case can shape public understanding for generations. Knowing this history helps us ask better questions and approach mental health conversations with more wisdom.
How Mental Health Legislation Impacts Diagnosis and Treatment
The Sybil controversy left a complicated legacy. But while the debate over that case still echoes, federal laws now shape how disorders like DID are actually treated in real life. These laws matter more than most people realize.
The biggest one is the Mental Health Parity and Addiction Equity Act, or MHPAEA. This federal law says that health insurance plans cannot treat mental health conditions worse than they treat physical ones.
According to the CMS overview of the Mental Health Parity and Addiction Equity Act, insurance companies must apply the same financial rules and treatment limits to mental health care as they do to medical or surgical care. For someone with dissociative identity disorder, this makes a real difference. It means a plan cannot cap therapy visits at six per year while allowing unlimited physical therapy. It means copays for a psychiatrist visit cannot be higher than copays for a cardiologist visit. The law creates a level playing field.
Before MHPAEA, many plans simply refused to pay for long term trauma therapy. They called it experimental or not medically necessary. Now, if your plan covers mental health at all, it must follow parity rules. The effect on DID treatment has been significant. More people can afford the sustained therapy needed to work through dissociation.
But the law does not fix everything. Involuntary commitment laws still vary wildly from state to state. When someone with DID enters a crisis and cannot keep themselves safe, the laws that determine what happens next depend entirely on where they live. Some states make it easy to get temporary hold orders and treatment. Others are much stricter. These differences affect whether a person gets timely help or falls through the cracks.
Confidentiality laws add another layer. HIPAA protects medical records at the federal level. But state privacy laws can offer stronger or weaker protections. For people living with DID, privacy is not a small concern. The stigma associated with multiple personality disorder still exists in 2026, even after the diagnosis changed names. Knowing that your treatment records stay private helps people feel safe enough to ask for help in the first place.
Understanding your legal rights is not just about bureaucracy. It is about knowing what you deserve from the system. If you want to learn more about how DID presents differently from other conditions, the resource on dissociative identity disorder symptoms and borderline personality disorder differences can help clarify what sets them apart.
Taking action on your own behalf starts with knowing the rules. Join An Experiment if you are ready to move from passive worry to active steps in your own wellness journey. And if you want to keep learning about topics like these, Join The Newsletter for ongoing updates that cut through the noise.
Key Federal Laws Every Patient Should Know
Beyond the basic protections of MHPAEA, two other federal laws create a powerful safety net for anyone living with multiple personality disorder.

The Affordable Care Act, or ACA, made mental health care an essential health benefit. That means most individual and small group plans must cover treatment for conditions like dissociative identity disorder. The Americans with Disabilities Act, or ADA, protects you from discrimination at work or in public spaces if your mental health condition qualifies as a disability.
Here is the catch. Even with these laws on the books, enforcement can be inconsistent. Recent actions by regulators have cracked down on insurance companies that still deny coverage unfairly. These enforcement moves highlight real gaps between what the law promises and what patients actually experience. Knowing your rights under each of these three laws changes the conversation. You can push back when a plan denies your claim. You can ask for accommodations at work. You can file complaints when your rights are violated.
If you want to understand the language used in mental health advocacy, the guide on mental health synonyms that build connection and reduce stigma can help you speak up more clearly. The power comes from knowing the rules and using them to get the care you deserve.
Stigma, Media Representation, and Public Perception of MPD
Knowing your legal rights is a powerful step. But the law only helps if you feel safe enough to use it. That is where stigma comes in. For anyone living with multiple personality disorder, the way the public sees the condition can be just as harmful as a denied insurance claim.

Hollywood has done a lot of damage here. Movies like Split and The Three Faces of Eve have shaped what most people think they know about MPD. And they have gotten it wrong. In these films, characters with multiple personalities are often violent, dangerous, or unpredictable. Research shows that inaccurate media portrayals of dissociative identity disorder directly lead to delays in seeking treatment, misdiagnosis, and increased shame. A 2024 study found that 129 out of 151 participants reported negative effects on their care because of how the disorder is shown on screen. You can read more about the negative impact of misportrayals of DID in media in the full study.
The most famous case is Sybil. The 1973 book and 1976 TV movie told the story of Shirley Ardell Mason, an art teacher who was said to have 16 personalities. The story helped make MPD a household term. But later investigations questioned whether the diagnosis was real or if it was created by a therapist who believed she had found something rare. The CBC article on who was Sybil and her multiple personalities explains how the case sparked a wave of diagnoses and controversy. Whether or not Sybil was accurate, the story set a template for how the public sees MPD. And that template is full of fear and drama.
Here is what that stigma costs real people. When the public believes people with MPD are dangerous, patients hide their symptoms. They avoid doctors. They lose jobs and friendships. They face discrimination in court and in clinics. The NAMI article on dissociative identity disorder as a misrepresented diagnosis points out that even mental health providers can be misled by dramatized portrayals. So patients end up fighting not just their own condition but also the misinformation everyone around them believes.
The good news is that things can change. Accurate media representation and public education make a real difference. When stories show MPD as a trauma response rather than a horror plot, people understand that those with the condition need help, not fear. If you want to learn what the actual symptoms look like and how they differ from other conditions, this detailed guide on dissociative identity disorder symptoms breaks it all down.
Stigma thrives in silence. The more we talk openly about what MPD really is, the harder it becomes for myths to survive. You can help push back against the stigma by staying connected to a community that values real understanding over sensational stories.
Join The Newsletter for ongoing updates on mental health topics, creative ways to take action, and a supportive space to keep learning.
And if you feel ready to move from passive reading into active change, you can always Join An Experiment and turn your curiosity into meaningful action alongside others who care about breaking down barriers.
The Role of Legislation in Protecting Patient Rights
Stigma does not just live in our heads or in Hollywood scripts. It also lives in courtrooms, insurance offices, and hospital intake forms. That is why laws exist to protect people with multiple personality disorder from discrimination and to make sure they get fair treatment. Knowing these legal rights can make the difference between getting proper care and being turned away.
One of the most important protections is confidentiality. For anyone with a complex trauma history, having control over who sees your medical records is critical. The Health Insurance Portability and Accountability Act, better known as HIPAA, gives you clear rights over your health information. You can ask to see your records, request corrections, and decide who gets to know about your diagnosis. The Your Rights Under HIPAA guide explains exactly what protections exist and how to file a complaint if those rights are violated. For someone living with multiple personality disorder, this means a therapist cannot share details of your treatment with family members or employers without your written permission. That is a big deal when fear of judgment keeps people from seeking help.
Beyond privacy, there is the issue of insurance coverage. For years, health plans could place stricter limits on mental health care than on physical health care. A person with multiple personality disorder could run out of covered therapy sessions long before someone with a physical illness ran out of doctor visits. The Mental Health Parity and Addiction Equity Act of 2008 changed that. This federal law requires group health plans to treat mental health benefits the same as medical and surgical benefits. Copays, deductibles, visit limits, and prior authorization rules must all be equal. The Mental Health and Substance Use Disorder Parity page from the Department of Labor breaks down what this means in plain language. If your insurance company charges higher copays for therapy than for a physical exam, that could be a violation of the law.
Patient advocacy organizations play a big role here too. Groups like NAMI and the National Disability Rights Network work to influence policy and push back against discrimination. They help shape how laws are enforced and make sure people with conditions like multiple personality disorder are not left out of protections. Recent legal cases have also set important precedents. Courts have ruled that severe mental health conditions qualify for disability protections under the Americans with Disabilities Act. That means employers cannot fire or refuse to hire someone simply because they have a diagnosis.
Understanding the words we use matters in legal contexts too. The term multiple personality disorder and its synonyms carry weight in court documents, insurance claims, and medical records. Using accurate language can affect whether a claim is approved or denied. For a closer look at how language shapes understanding, this guide on mental health synonyms that build connection shows how the right words can reduce stigma and improve communication with providers.
The bottom line is that the law offers real protection. But those protections only work when people know they exist. Learning your rights under HIPAA and the parity act is the first step. The next step is using them.
Current Trends and Future Directions in Policy and Research
The legal protections we just covered are already in place. But the world of mental health care does not stand still. Researchers, policymakers, and advocates are all working on what comes next. Understanding these trends helps you know what to expect and how to push for better care.
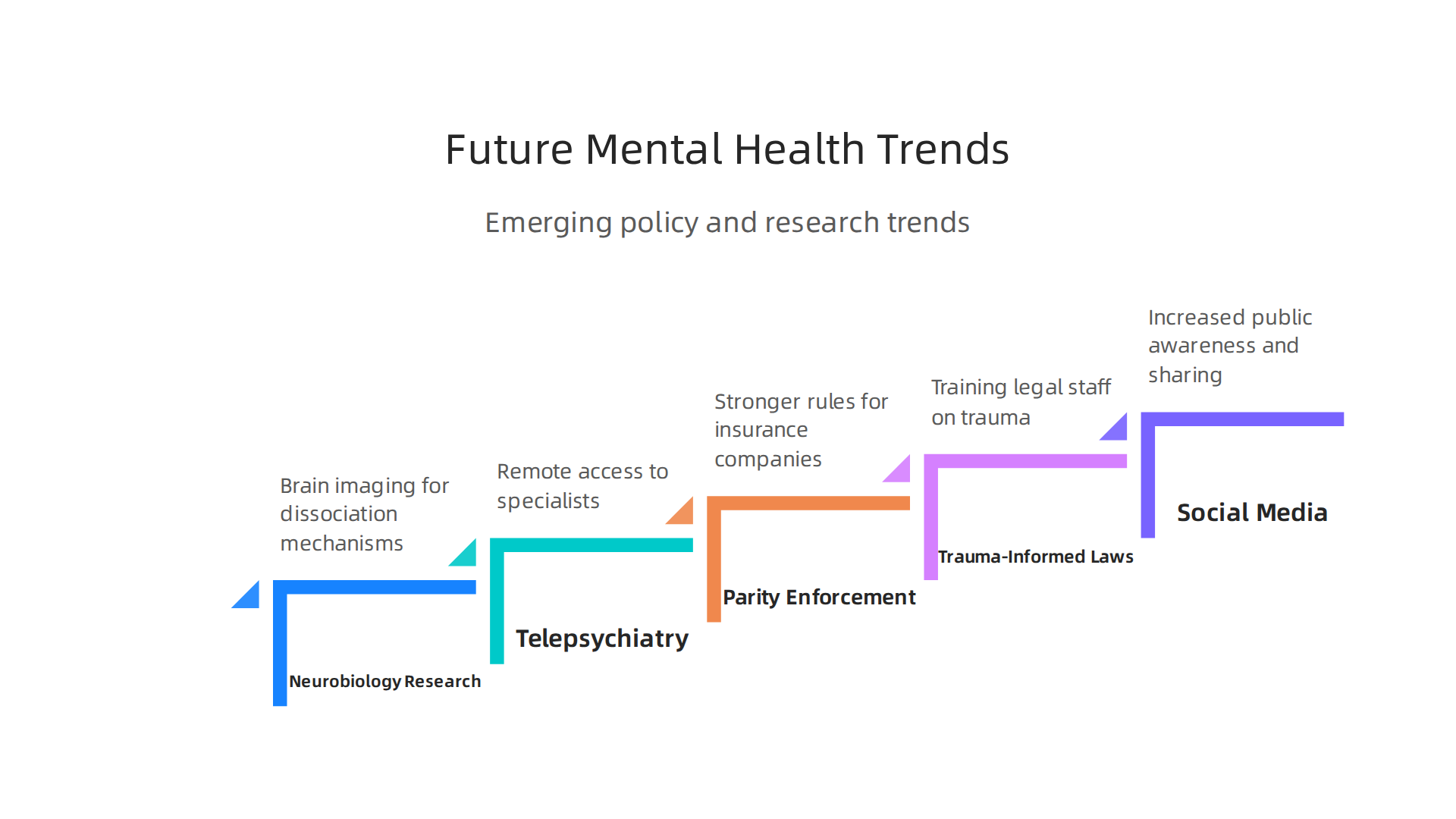
One of the most exciting areas is research into the neurobiology of dissociation. Scientists are using brain imaging to study what happens inside the brain when someone switches between identities. This research could lead to more accurate diagnostic tools and treatments that target the root causes.
The current diagnostic criteria are based on observable behaviors and self-reported symptoms, as outlined in the DSM-5. But future tools might include biological markers. For a deeper look at how the DSM-5 defines the condition, this guide on dissociative identity disorder diagnostic criteria explains the latest standards.
Policy trends are also heading in a positive direction. Telepsychiatry has grown a lot since 2020, and in 2026 it remains a key way for people with multiple personality disorder to reach specialists who understand dissociation. This is huge for people in rural areas or those who cannot travel. Lawmakers are also getting better at enforcing mental health parity rules. Insurance companies face more scrutiny when they try to limit therapy sessions or charge higher copays for mental health care. The push for parity is not done yet, but it is moving forward.
Advocacy movements are pushing for trauma-informed legal frameworks. This means training judges, lawyers, and court staff to understand how trauma affects memory and behavior. For someone with multiple personality disorder, this could change how their case is handled in family court or disability hearings. Advocacy groups argue that the legal system has a long way to go, but progress is happening.
Social media and public awareness are also shifting the conversation. More people are sharing their experiences with dissociation online. This helps reduce stigma and pushes researchers to focus on real patient needs. If you want to understand how multiple personality disorder differs from other conditions, this article on dissociative identity disorder vs borderline personality disorder breaks down the key differences.
All of these trends point to one thing: the future is getting better for people living with multiple personality disorder. Research is smarter, laws are fairer, and more people are listening.

The best way to stay informed and connected is to follow the groups and advocates doing the work.
If you want to keep learning about mental health rights, research updates, and ways to connect with a supportive community, Join The Newsletter for ongoing insights and stories.
Summary
This article clears up myths about